
For decades, exposure and response prevention (ERP) has been described as the “gold standard” for OCD. Yet the field of psychotherapy has a long history of declaring winners too early.
Budd and Hughes (2009) reminded the field that psychotherapy research faces an inherent difficulty: treatments are rarely isolated enough to determine whether one approach is universally superior. This problem became central to what is known as the Dodo Bird Verdict, a reference to the dodo character in Alice in Wonderland who, after an arbitrary race, declares that “everybody has won.” In psychotherapy research, the metaphor was adopted when studies that directly compared different therapies kept finding similar results, even though the treatments were based on very different ideas. Some interpreted this to mean that comparative treatment research was essentially “dead,” much like the extinct dodo itself, because our designs were rarely sensitive enough to detect meaningful distinctions.
With this context, Budd and Hughes’ warning becomes clear: when trials are designed as if “treatment type” were a stable, isolatable variable, the methodology itself limits what we can detect. The results may resemble the Dodo Verdict not because treatments are equivalent, but because the tools used to compare them were never built to reveal meaningful differences.
This does not mean that randomized controlled trials are unhelpful. RCTs are essential for showing whether a treatment works at all, whether it outperforms placebo or performs comparably to established interventions. But once effectiveness has been established, an absence of difference in group outcomes when compared with other treatments does not mean the treatments are identical or that they work equally well for everyone. A group-level tie does not imply that every individual responds equally well to every intervention.
Yet in OCD, this important distinction is rarely applied consistently. Instead of recognizing these limitations, the field often draws the opposite conclusion: ERP’s longstanding position must reflect an uncontested scientific victory. The absence of large differences is then reinterpreted as evidence that no new treatment is needed.
And when alternative approaches begin to show promise, such as inference-based cognitive-behavioral therapy (ICBT), their developers are not met with curiosity but with accusations of bias or overinvestment. The irony is hard to miss, because these accusations often reveal the very allegiance they aim to critique.
When the call of “bias” only goes one way
It is striking how readily researchers involved in ICBT are accused of bias, while allegiance to ERP is treated as a neutral scientific position. As the principal co-developer of ICBT, I am often the target of these claims, yet the characterization does not match the reality of how the evidence base was built. Although early work naturally came from our group, as is true for every new therapeutic model, ICBT outcome studies have been conducted across multiple sites, by researchers from varied theoretical backgrounds, and in independent labs not affiliated with its developers (Aardema et al., 2022; Visser et al., 2015; Wolf et al., 2024). Much like later ERP studies, these projects also included collaborators whose primary allegiances lay outside the model entirely. These collaborators may not include the highly visible ERP advocates who dominate podcasts and public commentary, but scientific credibility has never depended on media presence. They are established investigators, and their findings repeatedly converge. Under such conditions, the accusation of isolated, idiosyncratic developer bias becomes increasingly difficult to sustain.

Some of our trial clinical psychologists at the holiday dinner of the Obsessive Compulsive Disorders Clinical Study Center in Montreal. Most practice ERP, some practice ICBT, and all contribute to the research and common goal to improve outcomes for those with OCD.
But even correcting these misconceptions do not address the deeper issue. The real problem is the selective use of the bias argument. Allegiance in psychotherapy research does not reside only in authorship; it emerges through the interpretive norms of the field, the expectations about which mechanisms “should” matter, how improvement “ought” to be conceptualized, and which frameworks define the reference point for evaluating new ideas.
Because ERP has occupied the dominant position for decades, its assumptions have shaped the broader research culture. This influence is subtle but powerful: it affects how findings are interpreted, which hypotheses are considered legitimate, and how departures from the established model are judged. These cultural forces predate any individual trial and influence how all subsequent research is received, regardless of who conducted it.
Once we acknowledge these broader dynamics, the notion that ERP occupies a position of “neutrality” while ICBT is uniquely biased becomes impossible to defend. What is often labeled ‘bias’ in ICBT reflects something different: discomfort with alternatives that challenge longstanding assumptions. The reaction says less about the new therapy and more about the field’s attachment to the familiar.
This selective logic resurfaces in another common argument: the claim that adding cognitive therapy to ERP provides “no additional benefit,” and therefore cognitive methods must be unnecessary.
All treatments are equal, but some are more equal than others
A familiar argument from older studies is that adding cognitive therapy to ERP does not appear to improve outcomes, given the absence of significant differences in head-to-head comparisons. From this, some conclude that cognitive methods must be unnecessary. Yet the inference drawn is remarkably one-directional. If the combination is non-additive, the equally valid inverse conclusion is that ERP adds nothing to CT. That interpretation is almost never entertained.
This asymmetry reflects a broader pattern highlighted in the Dodo Bird discussion: when our methods are not designed to detect differences cleanly, the absence of difference tends to be interpreted in a way that protects existing assumptions. In this case, the “everybody has won” logic is applied selectively, always in favor of the dominant model.
The result is not a scientific conclusion but an interpretive habit. ERP becomes the presumed essential ingredient; CT becomes the optional accessory. Yet this is a conceptual leap rather than an empirical rule. A therapy’s identity derives from its theoretical foundation and the specific problem it is designed to solve.
The idea that CBT is not “really CBT” unless ERP is included is simply incorrect. Behavioral therapy can be behavioral without ERP. Cognitive therapy does not need exposure to qualify as CBT. What defines a treatment is its underlying model and mechanism, not the presence or absence of a particular technique. The category does not collapse merely because exposure is absent.
ICBT, in particular, is not defined in relation to exposure because it addresses a different problem altogether. I expand on this in a separate blog, “Why ICBT is not exposure by another name.” ICBT focuses on the reasoning process that constructs obsessional doubt at its origin. ERP, by contrast, works downstream, helping individuals learn from their reactions once doubt is already active. ICBT intervenes at the inferential and imaginative processes that generate doubt. ERP does not.
This is not a minor procedural distinction; it is a difference in purpose. And when purpose diverges, non-additivity tells us nothing about necessity, only that the comparison may not have been asking the right question.
Dead dodos, old assumptions, and new directions
Several authors have argued that the research field may need a broader lens. Leichsenring and colleagues (2019) called for a paradigm shift away from rigid comparisons of predefined treatment packages and toward the contextual factors that influence treatment success for different individuals. Cuijpers and collaborators (2025) recently emphasized that major breakthroughs rarely come from a single innovation. Instead, multiple incremental advances accumulate over time, particularly when we consider how different treatments can help different subsets of patients respond or remit.
This perspective aligns well with current work in OCD. The goal is no longer to crown a universal first-line treatment, because that question may be ill-posed. Treatments differ in mechanisms, in demands, and in the way clients relate to them. Matching people to what fits them, rather than forcing uniformity, is far more consistent with scientific progress.
For example, ICBT may help individuals whose difficulties stem primarily from inferential confusion, when imagination overrides perception and a hypothetical scenario feels more convincing than direct sensory evidence. Someone whose difficulties arise more squarely from fear-learning mechanisms may respond better to ERP. These observations are not competitive. They describe complementarity, not rivalry.
Offering more than one validated treatment is not a threat to ERP. It is an attempt to improve outcomes. The claim that no new treatment is needed reflects allegiance, not evidence. ICBT did not emerge in opposition to ERP. It emerged from investigating how obsessional doubt is reasoned into existence, a process distinct from the one ERP addresses.
Why integrating everything into one model can backfire
When a field grows around a single dominant model, it gradually develops a gravitational pull. New approaches are not first evaluated for what they are, but for how closely they resemble the prevailing framework or how easily they can be absorbed into it. In OCD, that gravitational center has long been ERP. As a result, when approaches such as ICBT, metacognitive therapy (MCT), Acceptance and Commitment Therapy (ACT), appraisal-based interventions, or mindfulness-based methods begin to demonstrate value, they are often filtered through a narrow question: How does this fit into ERP? And if it does not fit, can it be dismissed?
On the surface, this can seem pragmatic, an attempt to strengthen an established model by absorbing promising elements from elsewhere. But the instinct to fold everything into ERP risks undermining the very advantage these alternative frameworks provide. Treatments differ not just in techniques, but in mechanisms, conceptual foundations, and the pathways through which change occurs. ERP recalibrates fear learning. ICBT targets the reasoning processes that generate obsessional doubt. ACT emphasizes psychological flexibility. MCT addresses metacognitive style. Appraisal-based approaches focus on meaning-making. Mindfulness-based methods train attentional processes.
Many of these models struggled to gain visibility not only because their early evidence bases were small or still developing, but because they also faced additional, unnecessary headwinds. In a field organized around a single “first-line” treatment, genuinely distinct ideas often receive little oxygen. Novel approaches are expected to justify themselves against assumptions shaped by the dominant model, long before they are evaluated on their own terms.
Some individuals resonate with ACT’s values-based flexibility. Others connect with MCT’s attention to higher-order thinking processes. Others find mindfulness’s attentional training intuitive. These preferences, and the differential effects that may accompany them, arise precisely because each treatment maintains its own identity rather than being absorbed into ERP. When everything is folded into one dominant model, we risk creating a theoretical melting pot in which none of the original mechanisms remain coherent.
A therapy built from multiple models is not inherently stronger. Without a clear theoretical foundation, it risks losing the precision that makes it effective. If everything becomes ERP with scattered “cognitive elements,” or ICBT with incidental “exposure-like components,” we lose the ability to study mechanisms cleanly, and the treatments themselves risk becoming unrecognizable.
This dilution may not be benign. Some individuals may benefit exactly because a treatment preserves its distinct focus, whether on reasoning, learning, inference, flexibility, or attentional processes. Flattening these differences in the name of integration may unintentionally reduce effectiveness for the very clients who need alternatives most.
The field advances not by blending all therapies into a single hybrid, but by understanding what makes each validated treatment effective on its own terms. Distinctiveness is not a liability. It is a resource. It broadens clinical choice, supports better treatment matching, and preserves the diversity of mechanisms that may be essential for recovery.
Many roads lead to Rome, but not all roads are roads
A natural question follows from recognizing that different treatments rest on different mechanisms: why might different validated therapies help different people in different ways? At this stage, we do not have a definitive answer, but several plausible explanations exist.
One possibility is simple fit. Therapies, much like therapists, have personalities. Some clients resonate with exposure-based work because the behavioral logic feels intuitive. Others connect more deeply with reasoning-based approaches because these speak directly to how doubt forms and feels. Fit is not merely technical; it involves meaning, engagement, and whether the method aligns with how a person makes sense of their own experience.
Another possibility is that the mechanisms themselves differ. Not all treatments produce change through the same pathways. Some improvements may stem from inhibitory learning, others from shifts in attention, from changes in appraisal, or from resolving a reasoning process that created the problem. These internal pathways do not always map neatly onto symptom scores, and research is still clarifying how they operate.
This is also where the diversity of treatment models matters. ACT’s emphasis on values and psychological flexibility, MCT’s focus on how one relates to thinking, and mindfulness-based methods’ cultivation of attentional stability all offer distinct entry points for change. People often gravitate toward these frameworks not because they mimic ERP or ICBT, but because they maintain their own identity. Distinctiveness allows clients to find what resonates. When models are absorbed into a single dominant framework, the mechanisms that make them helpful can be diluted or lost.
Ultimately, these possibilities point toward research rather than premature conclusions. Over time, empirical work will help us determine which mechanisms matter most, why individuals respond differently, and how these insights can guide effective treatment matching.
Acknowledging diversity in mechanisms and fit does not imply that every new idea should be accepted uncritically. The Dodo Bird debate never claimed that all therapies are equivalent. It highlighted that our methods often struggle to detect meaningful differences. This is why rigorous validation remains essential. Randomized controlled trials, including head-to-head comparisons, are the backbone of responsible innovation. New treatments must demonstrate that they are at least as effective as existing approaches and/or that they offer distinct advantages for some individuals.
People vary, but not every path leads somewhere worth going. Some treatments lead to Rome; some lead nowhere. Evidence tells us which is which. The fact that individuals vary does not justify lowering standards or embracing untested therapies. As I have argued in another blog, the popularity or narrative appeal of approaches such as Brainspotting or Internal Family Systems is not evidence of effectiveness. Appeals to “everyone is different” do not excuse abandoning scientific rigor. A therapy must show, through careful research, that it reliably reduces symptoms and performs at least as well as existing benchmarks. Without that foundation, it is simply not a road worth traveling.
When a new treatment is validated, the field grows. Options expand. And the longstanding assumption that recovery must follow a single route becomes harder to defend. Once multiple treatments are recognized as scientifically grounded, the question shifts from “which therapy is best overall?” to the more clinically relevant: which therapy works best for whom, and under which conditions?
A new kind of trial: beyond head-to-head comparisons
This brings us to our most recent stepped-care trial at the Obsessive-Compulsive Disorders Clinical Study Center in Montreal. This is a publicly funded study registered with the U.S. National Library of Medicine at the National Institutes of Health (ClinicalTrials.gov identifier NCT06318806). Instead of asking which therapy is “better,” the study examines how different treatments can be sequenced to help those who do not reach remission with one approach alone.
In this design (see graph), all participants begin with ERP. This starting point should not be interpreted as an endorsement of ERP as a “first-line” intervention on theoretical or mechanistic grounds. Rather, it reflects the pathway most individuals with OCD typically encounter when they enter evidence-based care in routine clinical practice. ERP is currently the most widely available empirically supported intervention in everyday settings, and beginning with ERP allows the trial to mirror the treatment trajectory many patients follow once they access evidence-based approaches. Starting here maximizes generalizability and ensures that the findings can be applied to typical clinical contexts. A design that began with I-CBT and then stepped to ERP would be equally valid scientifically, but it would be less representative of prevailing patterns of evidence-based care.
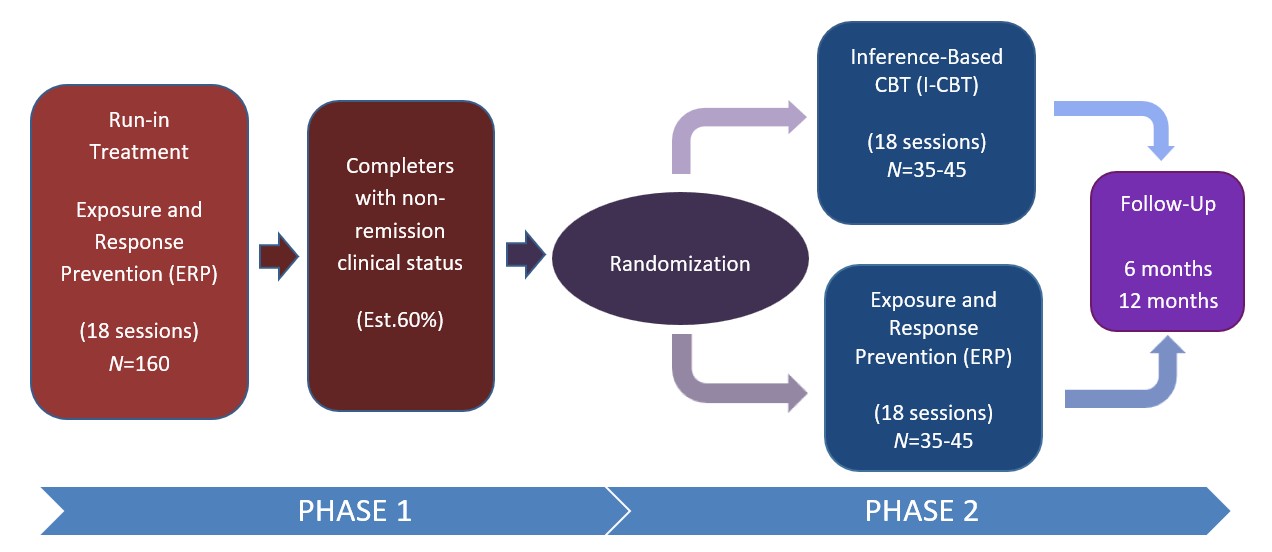
Those who do not reach remission then enter Phase 2, where they are randomized to receive either Inference-Based CBT (ICBT) or an additional course of ERP.
This is not a superiority trial. It is a matching trial, structured to answer a far more clinically relevant question:
Which treatment works best for which individuals, and at what point in their course of care?
The study also includes a predictive component. By examining early clinical and psychological markers, we hope to make a beginning with determining whether it is possible to anticipate who is likely to benefit from ERP and who may be better served by a reasoning-based intervention like ICBT. If such patterns can be identified, treatment can be matched earlier, reducing delay and improving overall remission rates.
The purpose is not to elevate one treatment above another. It is to understand how different people recover through different mechanisms and how we can offer each individual the approach that fits them best.
The dodo is not extinct after all
Perhaps the deeper message of the Dodo Bird debate is not that all treatments are identical, but that our lens has been too narrow. When the field assumes that one treatment must reign supreme, it overlooks the complexity of human reasoning, the diversity of obsessional doubt, and the scientific value of cultivating more than one well-validated road to recovery.
Accepting that multiple treatments can be effective in their own right does not mean relinquishing debate. It means strengthening it. The field will continue to wrestle with which mechanisms matter most, which pathways are more efficient or more durable, and which features of OCD are essential to target. These disagreements are not signs of fragmentation; they are the lifeblood of scientific progress. A field without such debate is not unified. It is stagnant.
The same holds for allegiance. Every therapeutic model has its champions; that is not bias but expertise. Calling ICBT biased simply because its researchers believe in the model is an unusual standard. Nearly every treatment in psychotherapy was developed, refined, and initially tested by people who understood it best. The double standard becomes visible only when the appearance of an alternative evokes defensiveness. When a new therapy is treated as a threat, the anxiety belongs not to the new treatment but to the field’s investment in the old one.
The critique that ICBT has been “managed too tightly” falls into a similar category. Preserving theoretical coherence is not gatekeeping. It is how scientific models remain testable, interpretable, and falsifiable. What sometimes looks like “siloing” reflects a simpler reality: much of ICBT’s development occurred over decades outside the ERP-centered spotlight. As the work has finally gained visibility, some observers have expressed surprise and mistakenly attributed the prominence of the developers’ names in research articles to bias, rather than to the inevitable outcome of having carried out sustained work in an area the broader field had largely neglected.
If there is a bias here, it lies not with the researchers who sustained the work, but with the historical absence of broader engagement.
Seen in this light, ERP and ICBT are not adversaries but different roads shaped by different understandings of OCD’s core mechanisms. ERP helped the field take important steps. ICBT adds further steps by addressing the reasoning processes that give rise to obsessional doubt. Both matter. Neither invalidates the other. And the existence of more than one validated treatment is not a sign of fracture; it is a sign of progress.
Different people need different treatments. The goal is not to defend a favorite model or preserve a hierarchy.
The goal is to help more people recover through whichever scientifically grounded road gets them there.
References
Aardema F, Bouchard S, Koszycki D, Lavoie ME, Audet JS, O’Connor K. (2022). Evaluation of Inference-Based Cognitive-Behavioral Therapy for Obsessive-Compulsive Disorder: A Multicenter Randomized Controlled Trial with Three Treatment Modalities. Psychotherapy and Psychosomatics, 91,348-359.
Budd R, Hughes I. (2009). The Dodo Bird Verdict–controversial, inevitable and important: a commentary on 30 years of meta-analyses. Clinical Psychology and Psychotherapy, 16, 510-22.
Leichsenring F, Steinert C, Ioannidis JPA (2019). Toward a paradigm shift in treatment and research of mental disorders. Psychological Medicine, 49, 2111-2117.
Cuijpers P, Harrer M, Furukawa T. Assessing the strength of innovations in the treatment of depression (2025). British Journal of Psychiatry, 227:1-4. doi: 10.1192/bjp.2025.98. Epub ahead of print.
Visser HA, van Megen H, van Oppen P, Eikelenboom M, Hoogendorn AW, Kaarsemaker M, van Balkom AJ. (2015). Inference-Based Approach versus Cognitive Behavioral Therapy in the Treatment of Obsessive-Compulsive Disorder with Poor Insight: A 24-Session Randomized Controlled Trial. Psychotherapy and Psychosomatics, 84, 284-93.
Wolf N, van Oppen P, Hoogendoorn AW, van den Heuvel OA, van Megen HJGM, Broekhuizen A, Kampman M, Cath DC, Schruers KRJ, van Es SM, Opdam T, van Balkom AJLM, Visser HAD (2024). Inference-Based Cognitive Behavioral Therapy versus Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder: A Multisite Randomized Controlled Non-Inferiority Trial. Psychotherapy and Psychosomatics, 93, 397-411.
© Frederick Aardema, PhD.— The Doubt Illusion Blog (2025)
